Strategic directions at the intersection of cryobiology and geroscience
*Correspondence to:
Rebecca D. Sandlin, Center for Engineering in Medicine & Surgery, Department of Surgery, Massachusetts General Hospital, Harvard Medical School, and Shriners Children’s Boston, Boston, MA 02129, USA.
E-mail: rdsandlin@mgh.harvard.edu
Geromedicine. 2026;2:202605. 10.70401/Geromedicine.2026.0026
Received: February 05, 2026Accepted: May 20, 2026Published: May 21, 2026
This article belongs to the Special lssue Understudied Directions in Aging Biology, Quantitative and First-Principles Approaches
Abstract
Cryobiology and geroscience share complementary goals in understanding and mitigating biological damage. Cryopreservation enables the long-term storage of living cells, tissues, and organs, with direct applications in aging-related interventions requiring transplantation, cell therapies, and regenerative approaches. Advances in cryopreservation technologies may expand biobanking of viable specimens across the lifespan, thus facilitating studies of aging phenotypes, biomarker discovery, drug screening, and therapeutic development. Notably, cryoinjury and biological aging share several common molecular features, including oxidative stress, DNA damage, protein misfolding, and mitochondrial dysfunction. These parallels suggest that repurposing geroscience-informed interventions may improve preservation outcomes by enhancing cellular resistance to cryogenic stress and post-thaw recovery. Here, representative opportunities at the interface of cryobiology and geroscience are summarized, emphasizing bidirectional strategies that may advance both fields. This Perspective builds upon discussions from the 2025 Quantitative Approaches and Understudied Questions in the Biology of Aging Workshop (Paris, France).
Keywords
Cryopreservation, transplantation, biobanking, cryoinjury
1. Introduction
The field of cryobiology studies the effects of low temperatures on biological systems. It aims to understand and control the complex physical and biochemical processes that occur during cooling, storage, and rewarming. Cryobiology is a highly translational field, in which developed procedures enable the storage of living biological specimens, including cells, tissues, organs, and even whole organisms, at low temperatures. The biological utility of cryopreservation arises from its effects on cellular metabolism, such that each 10°C reduction in temperature slows metabolic activity by approximately half[1]. This principle has led to the development of several temperature-based storage strategies, where lower temperatures correspond to longer storage durations. Storage regimes span from hypothermic to cryogenic temperatures. Under cryogenic conditions, molecular motion and biochemical activity essentially cease, enabling a state of metabolic arrest that allows for potentially indefinite storage. This ability to preserve biological materials has direct relevance to aging medicine. For example, the demand for transplantation, cell therapies, and tissue engineering technologies is increasing, in part due to the rising burden of age-related diseases. Extending the storage duration and availability of these biological materials could help address limitations in these interventions.
An overlapping aim of cryobiologists and geroscientists is to understand, delay, or even stop biological processes. Although these fields employ different approaches and pursue unique objectives, there are compelling opportunities for collaboration. In this Perspective, opportunities at the interface of cryobiology and geroscience that may directly advance the health and longevity of aging populations are highlighted. The potential application of geroscience insights to inform and improve the development of cryopreservation procedures is also examined. While some of these approaches remain in the early stages of development, others may be ready for immediate application.
2. Opportunities
Several opportunities exist at the intersection of cryobiology and aging research. Here, two main areas of focus are described, as illustrated in Figure 1. First, the use of emerging cryopreservation technologies in the treatment of conditions prevalent among aging populations is examined. Second, the role of cryopreservation tools in advancing aging research is described, along with how insights from geroscience may inform cryobiology and reduce cryoinjury.
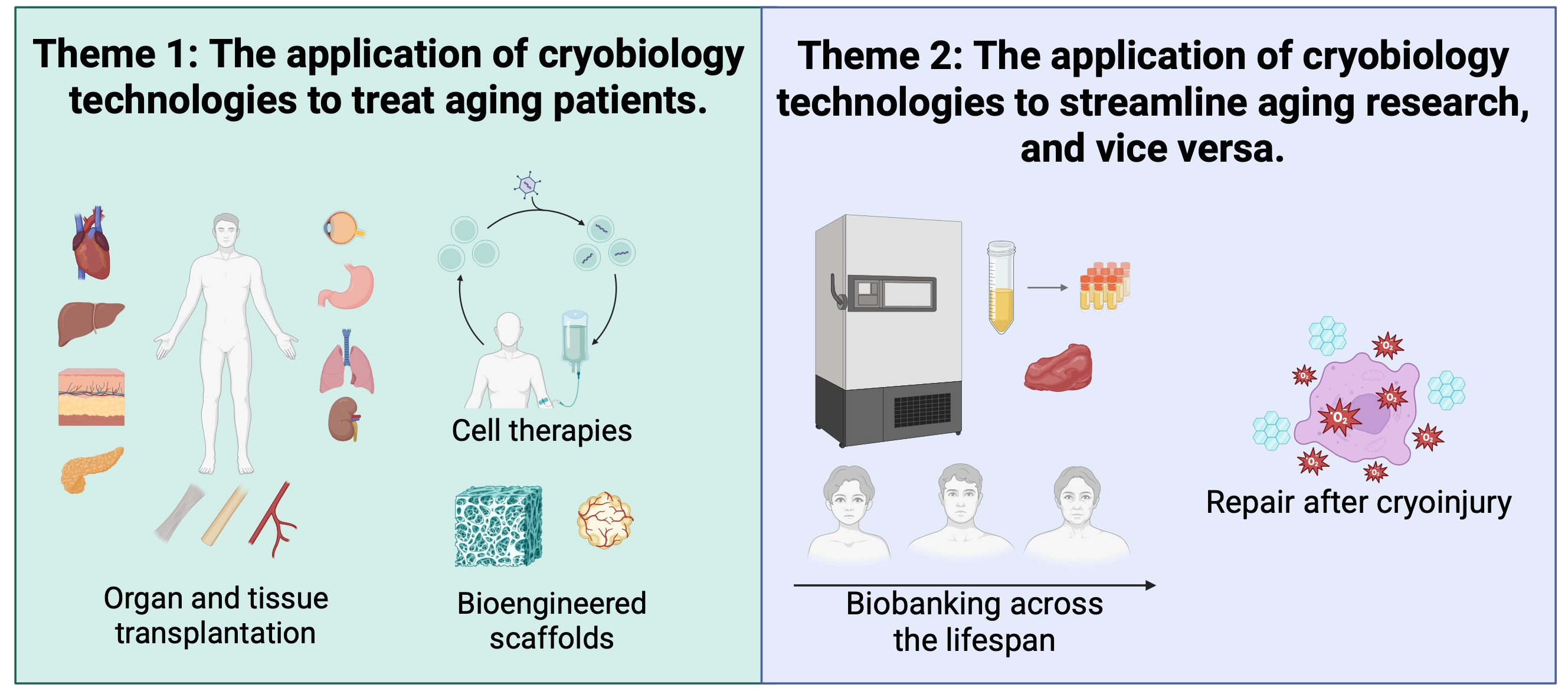
Figure 1. Overview of collaborative opportunities. Exemplary areas of overlap between cryobiology and geroscience are summarized. In Theme 1, cryopreservation and related preservation strategies support established clinical interventions and emerging approaches for treating conditions common in aging populations. This includes the cryopreservation of cell therapies, selected tissues, and ongoing efforts in organ preservation and banking. Theme 2 highlights bidirectional interactions between cryobiology and aging research. Cryopreservation enables biobanking of viable specimens and may support their use in single-cell, multi-omics, and functional studies. Conversely, insights from aging biology may inform strategies to mitigate cryoinjury and improve post-thaw recovery. Image created in Biorender.com.
2.1 Theme 1: Applications of cryobiology to treat aging patients
As populations age, morbidity associated with both physical trauma and chronic disease is expected to increase. This includes progressive atherosclerosis, stroke resulting from cerebrovascular degeneration, Alzheimer’s disease and other dementias associated with neurodegenerative processes, cancer arising from cumulative genetic damage, limb loss due to trauma or diabetes, and organ failure caused by progressive functional decline. Treatment of these conditions often requires a combination of medical therapy, surgical intervention, and supportive care. For advanced or end-stage conditions, organ transplantation or emerging regenerative approaches, such as cell-based therapies, may be required. Cryopreservation represents a core technology to streamline these interventions, enabling the storage, transport, and on-demand availability of living biological materials essential for treatment.
2.1.1 Organ, limb and tissue banking
Transplantation surgery has transformed modern medicine, enabling the replacement of failing organs, and more recently, complex tissues such as limbs, offering lifesaving and function-restoring outcomes that were once unimaginable[2]. During the 25-year period from 1987 to 2012, solid-organ transplantation was estimated to have restored over 2 million life-years to patients in the United States alone[3]. However, a key limitation is a shortage of donor organs, and it is estimated that up to one in five patients dies while on the waiting list[4]. One bottleneck is the short ex vivo shelf life of organs (~4-12 h). This leaves an extremely narrow window of time for logistical considerations and is a contributing factor to the organ shortage[5]. Cryopreservation has the potential to alleviate this bottleneck by extending storage time and reducing organ discard rates[4,6]. Additional storage time may be used to improve donor-recipient matching, provide greater flexibility for surgical preparation, and enable wider geographic sharing[4-6].
While cryopreservation may one day enable routine access to replacement organs and limbs, translation from cells to organs introduces significant challenges related to scale, physiology, and system complexity. The larger size of organs increases diffusion distances, which can result in non-uniform cryoprotectant distribution and increased toxicity. In parallel, heat transfer becomes a dominant issue, as temperature gradients during cooling and rewarming increase the risk of ice formation, devitrification, and thermomechanical stress, which can fracture the organ[7,8]. Despite these limitations, recent advances suggest large-scale organ cryopreservation may one day be possible. For instance, Tessier et al.[5] extended rat liver viability fivefold using high–subzero, nature-inspired storage strategies. Further, Han et al.[9] achieved successful cryopreservation of rat kidneys through ice-free vitrification. Supercooling has also been demonstrated to extend the viable storage time of human livers by 27 h[10]. These breakthroughs suggest that organ biobanks with “off-the-shelf” availability may become more feasible, potentially prolonging life and expanding access to organ transplantation. This approach may also be applied for the storage of limbs for vascularized composite allografts, tissues such as blood for transfusion[11], and pancreatic islets for transplantation[12]. However, scaling from rodents to human organs is a nontrivial challenge given the large differences in size, which impact cryoprotectant loading and heat transfer. Addressing these translational bottlenecks will be critical for enabling the clinical implementation of large-scale organ cryopreservation.
2.1.2 Cell therapies
Beyond whole-organ preservation, similar logistical and storage challenges arise in the delivery of cell-based therapies. Off-the-shelf availability of stem cells, immune cells, and engineered cell products could streamline logistics and broaden access to treatments for age-related diseases. These therapies show promise for cancer[13] and autoimmune disorders[13], and may also influence aging-related phenotypes[14], among others. With the prevalence of such conditions in older populations, cell therapies represent a promising approach to improve, manage, or potentially cure chronic diseases while preserving health and quality of life. Because these treatments rely on living cells, they are inherently constrained by limited shelf-life. These challenges may be especially pronounced when patients are geographically distant from manufacturing sites. Consequently, cryopreservation has been identified as a key element for the delivery of cell-based therapies[15]. Cryopreservation enables storage of both the primary tissue isolates and final cell products, facilitating distribution across sites. Cryopreservation helps ensure that the viability and functionality of the therapeutic product remain unchanged at the time of administration. Beyond enabling off-site preparation, cryopreservation supports later use of banked materials (e.g., cord blood), and eases logistics by allowing schedules to accommodate patients, donors, and clinical teams. Preservation strategies further facilitate the collection of autologous cells over multiple days or sessions when necessary[16]. While effective preservation methods exist for a range of cell therapies, several challenges remain. Reported protocols can cause cell loss, reduced viability, impaired cell attachment, altered metabolic activity, and phenotypic changes, which may negatively impact clinical outcomes[15-17]. Strategies to mitigate these effects include the optimization of non-toxic cryoprotectant formulations, and controlled cooling and thawing to limit ice damage. In addition, recovery might be improved through chemical supplementation targeting oxidative stress and mitochondrial dysfunction, as previously demonstrated in other systems[18]. Improved preservation strategies could enable global distribution and reduce manufacturing bottlenecks. They may also expand clinical trial participation and support the creation of large, diverse cell banks that represent multiple human leukocyte antigen (HLA) types. This could improve donor-recipient matching for allogeneic therapies. Together, these advances may expand access to cell-based treatments for aging populations.
2.1.3 Bioengineered constructs
Fabricated constructs combine living cells or bioactive molecules with engineered scaffolds. These systems hold promise for repairing or regenerating diseased or damaged tissues and organs, including skin and cartilage substitutes, bladder tissue, vascular grafts, heart patches, and liver organoids, among others[19-21]. Such constructs could transform the treatment of age-associated injuries and diseases, restoring function and improving quality of life. However, scaffold-based technologies that contain living cells will likely require robust cryopreservation procedures to ensure off-the-shelf availability and global transport. This procedure should maintain scaffold integrity and cell viability, enabling centralized production, batch consistency, scale-up, and global distribution. Effective preservation has already been demonstrated for several products, including StrataGraft®[19] and GRAFIX® Membranes for wound treatment. An emerging approach, temperature-controlled cryoprinting[22], involves printing cell-laden scaffolds directly onto a cryogenic substrate, integrating fabrication with immediate preservation. This approach has demonstrated successful fabrication and cryopreservation of 3D scaffolds using an alginate-collagen bioink. Cryoprinting may therefore eventually streamline the manufacture and storage of off-the-shelf engineered tissues such as skin grafts, vascularized patches, and organoids. By stabilizing constructs immediately after printing, this approach may help to maintain scaffold architecture and viability during storage and transport prior to clinical use. Beyond engineered tissues, this technology has recently been adapted for printing texture-modified food products for patients with dysphagia, a swallowing disorder common among aging populations[23]. While promising, future work in cryoprinting is needed to assess compatibility with additional bioinks and larger scaffolds. Long-term cryopreservation strategies will likely become essential for supply chain logistics in the production of bioengineered constructs. Cryopreservation may therefore support broader accessibility and more consistent therapeutic outcomes[24].
2.2 Theme 2: Bidirectional research across cryobiology and geroscience
Cryopreservation presents opportunities to advance aging research through the development of robust biobanks. Biobanks containing healthy and diseased biological materials serve as critical resources for studying disease mechanisms, developing diagnostics, and testing interventions[25-27]. In the context of aging, such repositories enable the systematic collection of biological snapshots across the human lifespan, supporting the identification of physiological and pathological changes over time[26]. Cryopreservation can therefore play an important role in aging research by providing researchers with the biospecimens they need when and where they are needed. Conversely, insights into the molecular drivers of aging may help inform strategies to mitigate cryoinjury and improve the post-thaw recovery. Because some forms of cryopreservation stress overlap mechanistically with natural aging, small molecules developed for geroprotective purposes could potentially be repurposed to reduce cryoinjury and enhance post-thaw viability of preserved specimens. This two-way interaction could accelerate advances across both fields.
2.2.1 Banking of diverse biological tissues as a catalyst for aging research
Biobanks are vital resources for scientific and medical research, housing specimens from both healthy individuals and patients, including saliva, blood, urine, solid tissues, and reproductive materials, among others[25-27]. These collections support drug discovery, diagnostic development, and studies of disease mechanisms. Such resources are increasingly integrated with single-cell and multi-omics technologies, enabling high-resolution characterization of molecular changes, including those relevant to aging[28-31]. Further, modern biobanks are now evolving to support the storage and recovery of viable and functional cells and tissues as opposed to only preserving analytes (e.g., DNA)[32]. This may allow for the recovery of biological specimens that are physiologically and biochemically comparable to their original states. Such samples could support molecular, functional, and structural studies using biologically intact materials[32]. For example, preserving functional brain tissue could advance research on neurodegenerative diseases such as Alzheimer’s and Parkinson’s diseases. Further, storing immune cells could support studies of autoimmune disorders and age-related changes in vaccine responsiveness. In parallel, banking tissue biopsies from aged organs could provide critical insights into late-life pathology. Finally, longitudinal studies of individuals or populations throughout their lifetime would be valuable to study the changes that occur over time, prior to onset of disease. Large-scale biobanking initiatives have already expanded worldwide, including major national programs in China[33], Europe[34], the United Kingdom[35], and the United States[36,37]. These efforts support precision medicine, aging research, and translational medicine through biospecimen collection, cryostorage, and the integration of clinical and molecular data. However, achieving the full potential of biobanking will require continued improvements in cryopreservation protocols to minimize cryoinjury and maintain native cellular function.
To fully leverage biobanking for aging research, continued improvements in cryopreservation and standardization of storage protocols will be required to ensure reproducibility and maintain cellular function across sites. This includes, at minimum, the selection of cryoprotectant formulations, control of cooling and rewarming rates, and post-thaw assessment of viability and function. In parallel, linking biobanked specimens to detailed clinical metadata, including patient demographics, longitudinal health data, and treatment histories, will be crucial for enabling meaningful translational insights. Large-scale longitudinal cohorts such as the Nurses’ Health Study have demonstrated the value of combining biospecimen collection with detailed clinical and lifestyle data. These efforts have generated insights into chronic disease risk and prevention[36]. This approach is further illustrated by the UK Biobank[35], which contains biological samples linked to health data from more than 500,000 participants and serves as an open-access resource for discovery. However, expanding these models to include viable cell and tissue resources remains an ongoing opportunity that will require continued advances in cryopreservation technologies.
2.2.2 Treatment of cryoinjury using geroscience tools
Following cryopreservation, biospecimens may exhibit oxidative stress, DNA damage, protein denaturation, mitochondrial dysfunction, and other injuries that lead to apoptosis, cell death, or impaired function[38-40]. These stress responses mirror many of the molecular hallmarks of aging, such as genomic instability, loss of proteostasis, and mitochondrial dysfunction[41,42]. An emerging approach to reduce the impact of cryoinjury involves chemical supplementation to target pathways of deterioration[43,44]. This approach aims to mitigate multiple forms of cellular stress that arise during cooling, storage, or rewarming.
Molecular studies of damage following subnormothermic or cryogenic storage have implicated cellular stress pathways and regulated cell death processes. Oxidative stress, in particular, is a consistent feature across storage conditions, with increased reactive oxygen species (ROS) contributing to cell death and loss of function[45-47]. Treatment with antioxidants such as melatonin[48], resveratrol[49], coenzyme Q10[50], quercetin[51], reduced glutathione[52], N-acetylcysteine[53], and Vitamin E[54], has been shown in some systems to improve the viability and functional recovery of specimens after storage[46,55]. For example, a study by Taylor et al.[56] demonstrated that supplementation of human sperm cryopreservation medium with a vitamin E analog significantly enhanced post-thaw motility, suggesting mitigation of freeze-thaw-induced oxidative cryoinjury. While the precise molecular mechanisms are not fully understood, oxidative stress in cryopreservation occurs acutely during freeze-thaw transitions. ROS generation may arise from opening of the mitochondrial permeability transition pore, leading to electron leakage, with additional contributions from stress-activated oxidase systems[46,55]. In aging, oxidative stress develops chronically through processes such as mitochondrial DNA mutation accumulation, impaired mitophagy, and declining antioxidant defenses[57,58]. Cryopreservation can also activate stress-response signaling pathways, including mitogen-activated protein kinase (MAPK)-mediated responses and downstream apoptosis cascades. Chemical inhibition of p38 MAPK (SD-282) has been shown to improve viability and functional recovery of human islets following cryopreservation[59]. This same pathway has also been implicated in the aging of gut stem cells[60], Leydig cells[61], and age-related macular degeneration[62].
Cryoinjury is not limited to molecular damage but may also contribute to mechanical changes following cryopreservation. For example, a prior study by Venkatasubramanian et al. demonstrated that cryoinjury can alter the mechanical properties of arteries, with changes in stress-strain behavior observed after thawing[63]. The mechanisms responsible for these changes were thought to include damage to the extracellular matrix (ECM), loss of viability in smooth muscle cells, redistribution of water, or structural changes due to the presence of ice crystals[63]. Major physical changes may also be observed during vitrification, an ice-free approach to cryopreservation in which specimens are preserved in an amorphous glassy state rather than crystalline ice. Here, thermomechanical stress experienced during cooling and rewarming can lead to cracking or fracturing of the biospecimen[64]. The aging process has also been linked to mechanical changes in cells and the surrounding ECM, which may result in increased stiffness and reduced compliance over time[65]. These changes may be due to increased collagen crosslinking, elevated levels of matrix metalloproteinase-mediated degradation and remodeling, or accumulation of glycation products[65]. While the mechanisms underlying mechanical alterations may differ between cryoinjury and aging, both processes ultimately result in physical changes that may compromise structural integrity. Specifically, mechanical changes from cryoinjury occur acutely and are primarily due to physical stress associated with temperature changes or ice crystallization. Conversely, mechanical changes during aging occur gradually and are driven by biological mechanisms, including collagen crosslinking and the accumulation of advanced glycation end products.
Shared mechanisms between aging and cryoinjury provide a foundation for the development of targeted intervention strategies. While cryoinjury occurs acutely, biological aging-related stress typically arises gradually but may lead to similar downstream damage over time. Despite these differences in timescale and origin, geroscience-informed interventions may be relevant in cryopreservation. This may include nuclear factor erythroid 2-related factor (Nrf2) agonists to enhance antioxidant defenses[66,67], proteostasis-targeting strategies to reduce protein aggregation or misfolding[68], sirtuin activators to promote DNA repair and cellular stress resistance[69], or mitochondrial stabilizers to preserve mitochondrial function[70]. A major limitation, however, is that the complete molecular basis of cryoinjury remains unresolved. A clearer molecular understanding will be critical for identifying targeted intervention strategies. Nonetheless, overlapping forms of damage observed in cryoinjury and aging present opportunities for cross-disciplinary collaboration. Small molecules that enhance stress resistance could potentially be tested in cryopreservation systems. In principle, these interventions could prevent damage during storage and promote repair or rejuvenation after thawing, thereby improving recovery and functional outcomes.
3. Conclusions
While this Perspective highlights opportunities for collaboration across cryobiology and geroscience, the topics discussed remain at various stages of development. First, significant scientific and technical barriers must be addressed in large-scale organ cryopreservation. Advances in cryopreservation technologies will be required to scale from rodents to human organs, with major challenges arising from size-dependent differences in cryoprotectant diffusion and cooling and rewarming rates. As a result, clinical implementation of large-organ preservation will likely remain a longer-term objective requiring additional technical and translational advances. Second, a better understanding of the molecular mechanisms of cryoinjury is needed to identify shared pathways with aging. Such insights could support the rational repurposing of geroscience-informed small molecules and interventions to improve cryopreservation outcomes. Third, biobanking of viable and functional human cells and tissues is already being implemented and may continue to expand in the near term. However, improved cryopreservation protocols are necessary to preserve more complex materials, including functional brain tissue, and will require standardization to ensure reproducibility across sites. A possible translational pathway for the field will involve continued optimization and standardization of preservation methods for cells and simple tissues, in parallel with larger and more complex biological systems, including engineered tissues, patient-derived tissues, and ultimately human organs. Key milestones will likely include the development of low-toxicity cryoprotectants, improved cryoprotectant loading, mitigation of ice-related and thermomechanical stress during cooling and rewarming, standardized post-thaw functional assessment, and demonstration of reproducible recovery in increasingly complex specimens. Continued progress in these areas may help realize the collaborative potential of these fields in both research and clinical contexts.
Beyond scientific and technical challenges, there remain ethical considerations, particularly in the context of human tissue cryopreservation. Research on biobanking ethics highlights the need for ongoing governance and transparency, as well as safeguards to protect genetic privacy and manage incidental findings arising from stored tissues[71]. Questions also remain regarding equitable access to these technologies, the commercialization or commodification of human biological materials, and uncertainties surrounding long-term storage and stewardship[72,73]. In the context of organ and limb cryopreservation, these concerns are further complicated by issues related to allocation and prioritization, particularly if extended preservation times alter existing transplant waitlist systems[74]. Careful consideration of these issues will be essential as cryopreservation technologies continue to evolve and move toward broader clinical applications. This will likely require ethical frameworks emphasizing informed consent, transparent governance, equitable access, and long-term stewardship of cryopreserved biological materials[75].
Cryobiology and geroscience converge on a shared challenge: understanding and mitigating biological damage, albeit across vastly different timescales. Advances in cryopreservation have the potential to transform the storage and distribution of organs, tissues, and cell-based therapies, with direct implications for the treatment of age-related diseases. At the same time, the ability to preserve viable biological specimens enables new approaches to study the mechanisms of aging across the lifespan. Importantly, the mechanistic overlap between cryoinjury and biological aging presents an opportunity to translate insights across fields, where geroscience interventions could improve cryopreservation outcomes. Realizing this potential may strengthen connections between aging biology and preservation science, with implications for both research and clinical applications.
Acknowledgements
The author utilized ChatGPT (OpenAI) to improve the grammar and clarity of the final draft. The authors take full responsibility for the integrity, originality, and accuracy of the work.
Authors contribution
The author contributed solely to the article.
Conflicts of interest
Rebecca D. Sandlin holds issued and pending patents related to biopreservation technologies. No other competing interests to declare.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
Not applicable.
Funding
This work was supported by the National Science Foundation (Grant No. 2440587).
Copyright
© The Author(s) 2026.
References
-
2. Bezinover D, Saner F. Organ transplantation in the modern era. BMC Anesthesiol. 2019;19(1):32.[DOI]
-
3. Rana A, Gruessner A, Agopian VG, Khalpey Z, Riaz IB, Kaplan B, et al. Survival benefit of solid-organ transplant in the United States. JAMA Surg. 2015;150(3):252.[DOI]
-
4. Lewis JK, Bischof JC, Braslavsky I, Brockbank KGM, Fahy GM, Fuller BJ, et al. The Grand Challenges of Organ Banking: Proceedings from the first global summit on complex tissue cryopreservation. Cryobiology. 2016;72(2):169-182.[DOI]
-
5. Tessier SN, de Vries RJ, Pendexter CA, Cronin SEJ, Ozer S, Hafiz EOA, et al. Partial freezing of rat livers extends preservation time by 5-fold. Nat Commun. 2022;13(1):4008.[DOI]
-
6. Giwa S, Lewis JK, Alvarez L, Langer R, Roth AE, Church GM, et al. The promise of organ and tissue preservation to transform medicine. Nat Biotechnol. 2017;35(6):530-542.[DOI]
-
7. Chen J, Liu X, Hu Y, Chen X, Tan S. Cryopreservation of tissues and organs: Present, bottlenecks, and future. Front Vet Sci. 2023;10:1201794.[DOI]
-
8. Gangwar L, Han Z, Scheithauer C, Namsrai BE, Kantesaria S, Goldstein R, et al. Physical vitrification and nanowarming at liter-scale CPA volumes: Toward organ cryopreservation. Nat Commun. 2025;16(1):8511.[DOI]
-
9. Han Z, Rao JS, Gangwar L, Namsrai BE, Pasek-Allen JL, Etheridge ML, et al. Vitrification and nanowarming enable long-term organ cryopreservation and life-sustaining kidney transplantation in a rat model. Nat Commun. 2023;14(1):3407.[DOI]
-
10. de Vries RJ, Tessier SN, Banik PD, Nagpal S, Cronin SEJ, Ozer S, et al. Supercooling extends preservation time of human livers. Nat Biotechnol. 2019;37(10):1131-1136.[DOI]
-
13. Patel KK, Tariveranmoshabad M, Kadu S, Shobaki N, June C. From concept to cure: The evolution of CAR-T cell therapy. Mol Ther. 2025;33(5):2123-2140.[DOI]
-
14. Garay RP. Recent clinical trials with stem cells to slow or reverse normal aging processes. Front Aging. 2023;4:1148926.[DOI]
-
15. Meneghel J, Kilbride P, Morris GJ. Cryopreservation as a key element in the successful delivery of cell-based therapies: A review. Front Med. 2020;7:592242.[DOI]
-
17. Cottle C, Porter AP, Lipat A, Turner-Lyles C, Nguyen J, Moll G, et al. Impact of cryopreservation and freeze-thawing on therapeutic properties of mesenchymal stromal/stem cells and other common cellular therapeutics. Curr Stem Cell Rep. 2022;8(2):72-92.[DOI]
-
18. Ha SJ, Kim BG, Lee YA, Kim YH, Kim BJ, Jung SE, et al. Effect of antioxidants and apoptosis inhibitors on cryopreservation of murine germ cells enriched for spermatogonial stem cells. PLoS One. 2016;11(8):e0161372.[DOI]
-
19. Hoffman T, Khademhosseini A, Langer R. Chasing the paradigm: Clinical translation of 25 years of tissue engineering. Tissue Eng Part A. 2019;25(9-10):679-687.[DOI]
-
20. Han F, Wang J, Ding L, Hu Y, Li W, Yuan Z, et al. Tissue engineering and regenerative medicine: Achievements, future, and sustainability in Asia. Front Bioeng Biotechnol. 2020;8:83.[DOI]
-
23. Lou L, Bilbao-Sainz C. Temperature-controlled cryoprinting vegetarian food with modified macro- and microstructures for dysphagia. ACS Food Sci Technol. 2025;5(8):3219-3228.[DOI]
-
24. Budharaju H, Sundaramurthi D, Sethuraman S. Biofabrication & cryopreservation of tissue engineered constructs for on-demand applications. Biofabrication. 2024;16(4):042008.[DOI]
-
25. Gallagher CS, Ginsburg GS, Musick A. Biobanking with genetics shapes precision medicine and global health. Nat Rev Genet. 2025;26(3):191-202.[DOI]
-
26. Paskal W, Paskal AM, Dębski T, Gryziak M, Jaworowski J. Aspects of modern biobank activity–comprehensive review. Pathol Oncol Res. 2018;24(4):771-785.[DOI]
-
27. De Souza YG, Greenspan JS. Biobanking past, present and future: Responsibilities and benefits. Aids. 2013;27(3):303-312.[DOI]
-
28. Zhang S, Wang Z, Wang Y, Zhu Y, Zhou Q, Jian X, et al. A metabolomic profile of biological aging in 250, 341 individuals from the UK Biobank. Nat Commun. 2024;15(1):8081.[DOI]
-
29. Garg M, Karpinski M, Matelska D, Middleton L, Burren OS, Hu F, et al. Disease prediction with multi-omics and biomarkers empowers case–control genetic discoveries in the UK Biobank. Nat Genet. 2024;56(9):1821-1831.[DOI]
-
30. Li Y, Tang S, Wang H, Zhu H, Lu Y, Zhang Y, et al. A pancreatic cancer organoid biobank links multi-omics signatures to therapeutic response and clinical evaluation of statin combination therapy. Cell Stem Cell. 2025;32(9):1369-1389.e14.[DOI]
-
33. Walters RG, Millwood IY, Lin K, Schmidt Valle D, McDonnell P, Hacker A, et al. Genotyping and population characteristics of the China kadoorie biobank. Cell Genom. 2023;3(8):100361.[DOI]
-
34. Litton JE. Launch of an infrastructure for health research: BBMRI-ERIC. Biopreserv Biobanking. 2018;16(3):233-241.[DOI]
-
38. Gao D, Critser JK. Mechanisms of cryoinjury in living cells. ILAR J. 2000;41(4):187-196.[DOI]
-
39. Martin G, Sabido O, Durand P, Levy R. Cryopreservation induces an apoptosis-like mechanism in bull sperm. Biol Reprod. 2004;71(1):28-37.[DOI]
-
41. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013;153(6):1194-1217.[DOI]
-
42. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. Hallmarks of aging: An expanding universe. Cell. 2023;186(2):243-278.[DOI]
-
43. Murray KA, Gibson MI. Chemical approaches to cryopreservation. Nat Rev Chem. 2022;6(8):579-593.[DOI]
-
44. Varo-Ghiuru F, Miclea I, Hettig A, Ladoşi I, Miclea V, Egerszegi I, et al. Lutein, Trolox, ascorbic acid and combination of Trolox with ascorbic acid can improve boar semen quality during cryopreservation. Cryo Letters. 2015;36(1):1-7.[PubMed]
-
45. Liu X, Xu Y, Liu F, Pan Y, Miao L, Zhu Q, et al. The feasibility of antioxidants avoiding oxidative damages from reactive oxygen species in cryopreservation. Front Chem. 2021;9:648684.[DOI]
-
48. Yang J, Guo S, Pan B, Qazi IH, Qin J, Zang S, et al. Melatonin promotes in vitro maturation of vitrified-warmed mouse GV oocytes potentially by modulating MAD2 protein expression of SAC component through MTRs. Cryobiology. 2021;102:82-91.[DOI]
-
49. Comizzoli P, Wildt DE, Pukazhenthi BS. In vitro compaction of germinal vesicle chromatin is beneficial to survival of vitrified cat oocytes. Reprod Domest Anim. 2009;44(s2):269-274.[DOI]
-
51. Davoodian N, Kadivar A, Ahmadi E, Nazari H, Mehrban H. Quercetin effect on the efficiency of ovine oocyte vitrification at GV stage. Theriogenology. 2021;174:53-59.[DOI]
-
52. López M, Bollag RJ, Yu JC, Isales CM, Eroglu A. Chemically defined and xeno-free cryopreservation of human adipose-derived stem cells. PLoS One. 2016;11(3):e0152161.[DOI]
-
53. Sandlin RD, Wong KHK, Boneschansker L, Carey TR, Miller KL, Rose G, et al. Preservative solution that stabilizes erythrocyte morphology and leukocyte viability under ambient conditions. Sci Rep. 2017;7:5658.[DOI]
-
57. Finkel T, Holbrook NJ. Oxidants, oxidative stress and the biology of ageing. Nature. 2000;408(6809):239-247.[DOI]
-
59. Omori K, Valiente L, Orr C, Rawson J, Ferreri K, Todorov I, et al. Improvement of human islet cryopreservation by a p38 MAPK inhibitor. Am J Transplant. 2007;7(5):1224-1232.[DOI]
-
60. He D, Wu H, Xiang J, Ruan X, Peng P, Ruan Y, et al. Gut stem cell aging is driven by mTORC1 via a p38 MAPK-p53 pathway. Nat Commun. 2020;11:37.[DOI]
-
63. Venkatasubramanian RT, Grassl ED, Barocas VH, Lafontaine D, Bischof JC. Effects of freezing and cryopreservation on the mechanical properties of arteries. Ann Biomed Eng. 2006;34(5):823-832.[DOI]
-
65. Phillip JM, Aifuwa I, Walston J, Wirtz D. The mechanobiology of aging. Annu Rev Biomed Eng. 2015;17:113-141.[DOI]
-
66. Zhang H, Davies KJA, Forman HJ. Oxidative stress response and Nrf2 signaling in aging. Free Radic Biol Med. 2015;88:314-336.[DOI]
-
67. Mayer C, Riera-Ponsati L, Kauppinen S, Klitgaard H, Erler JT, Hansen SN. Targeting the NRF2 pathway for disease modification in neurodegenerative diseases: Mechanisms and therapeutic implications. Front Pharmacol. 2024;15:1437939.[DOI]
-
68. Labbadia J, Morimoto RI. The biology of proteostasis in aging and disease. Annu Rev Biochem. 2015;84:435-464.[DOI]
-
69. Bonkowski MS, Sinclair DA. Slowing ageing by design: The rise of NAD+ and sirtuin-activating compounds. Nat Rev Mol Cell Biol. 2016;17(11):679-690.[DOI]
-
71. Wolf SM, Crock BN, Van Ness B, Lawrenz F, Kahn JP, Beskow LM, et al. Managing incidental findings and research results in genomic research involving biobanks and archived data sets. Genet Med. 2012;14(4):361-384.[DOI]
-
73. Evers K, Forsberg J, Hansson M. Commercialization of biobanks. Biopreserv Biobanking. 2012;10(1):45-47.[DOI]
-
74. Capron AM, Pruett TL, Childress JF. The big chill: Opportunities for, and challenges to, advanced biopreservation of organs for transplantation. J Law Med Ethics. 2024;52(3):595-610.[DOI]
Copyright
© The Author(s) 2026. This is an Open Access article licensed under a Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, sharing, adaptation, distribution and reproduction in any medium or format, for any purpose, even commercially, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Publisher’s Note
Science Exploration remains a neutral stance on jurisdictional claims in published
maps
and institutional affiliations. The views expressed in this article are solely those
of
the author(s) and do not reflect the opinions of the Editors or the publisher.
Share And Cite



Science Exploration Style
Sandlin RD. Strategic directions at the intersection of cryobiology and geroscience. Geromedicine. 2026;2:202605. https://doi.org/10.70401/Geromedicine.2026.0026
Tips
Copy completed.
Submit a Manuscript
Author Instructions
Cite this Article
Article Metrics
0
View
0
Download
Cited
Article Updates

Science Exploration Style
Sandlin RD. Strategic directions at the intersection of cryobiology and geroscience. Geromedicine. 2026;2:202605. https://doi.org/10.70401/Geromedicine.2026.0026
copy
Share Link
copy